Umbilical hernias include para-umbilical, supraumbilical and epigastric hernias. These are all classed as primary ventral hernias, meaning they occur naturally. Incisional hernias, by contrast, are secondary ventral hernias and develop at the site of a previous surgical incision.
An umbilical hernia occurs in or around the belly button (navel), often causing a lump inside the navel to protrude. In some cases, the swelling appears just above the navel rather than directly within it. This is known as a supraumbilical hernia.
Where do these hernias occur?
Hernias can develop anywhere along the midline of the abdominal wall, from the navel up to the breastbone. When they occur higher up, they are known as epigastric hernias.
These hernias always form along the centre of the abdomen because they pass through the natural gap between the two rectus muscles. Although the lump may appear slightly to one side, the underlying weakness is always located in the midline.
What does an umbilical hernia look like?
An umbilical hernia usually appears as a bulge or lump inside the navel beneath the skin. It can vary greatly in size, from a small grape-sized swelling to a much larger bulge, depending on the size of the hole in the abdominal wall and how much tissue pushes through.
The lump may become more noticeable when standing, coughing, straining or lifting. In some cases, it may reduce in size when lying down.
Sites of umbilical hernias
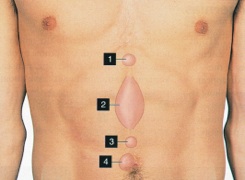
KEY
- Epigastric hernia
- Diastasis**
- Supraumbilical hernia
- Umbilical hernia
If it’s a hernia, what exactly is the lump?
The lump is usually fatty tissue that lies beneath the abdominal muscle and forms part of the body's natural padding. Sometimes, however, it may contain a portion of the intestine.
If intestine becomes trapped within the hernia, it can lose its blood supply. This is known as a strangulated hernia and requires urgent medical attention. (See Strangulated Hernia).
Repair the umbilical hernia or 'wait and see'?
You should repair it as soon as possible. Whilst these hernias can be relatively painless, if left alone they always enlarge.
Like all hernias, if left untreated they:
- run the risk of strangulating
- become more difficult to repair
(See also Is ‘No treatment’ an Option?)
What is the best umbilical hernia repair method?
This depends on the size of the hernia defect.
Those that are less than 1cm can often be repaired without mesh, using sutures that overlap the edges of the defect in a similar way to a double-breasted jacket. This produces a strong repair with a negligible risk of recurrence.
For defects larger than 1cm, mesh generally provides the most secure repair.
Our experience shows that the mesh should be placed beneath the defect, between the muscle layer and the lining of the abdomen (the peritoneum). This is known as the sublay technique.
Placing mesh on top of the muscle layer, known as the onlay technique, can lead to complications such as fluid collection beneath the skin and infection. This is another reason why mesh is often unsuitable for very small defects.
Open or keyhole repair for umbilical hernias?
Both techniques can work well. However, laparoscopic (keyhole) repair has several disadvantages:
- Laparoscopic surgery cannot be performed under local anaesthesia and requires a general anaesthetic.
- Three or more incisions are required to repair a single defect.
- The mesh used must be significantly larger than the hernia defect to achieve adequate overlap.
- In some cases, mesh may be placed inside the abdomen, which can lead to problems if the intestine adheres to it.
See also the section comparing Laparoscopic hernia repair and open mesh repair.
The British Hernia Centre
The British Hernia Centre is the UK's only dedicated specialist hernia centre, with over 37 years of expertise in hernia surgery. We have a proven track record and perform more hernia operations, including umbilical and supraumbilical hernias, than any other surgical unit worldwide.
If you have noticed a hernia by the navel, a lump inside the navel, or a supraumbilical hernia above the belly button, contact our team today to find out more or to arrange a consultation.
