The British Hernia Centre’s preferred method in most cases
A number of surgeons felt that none of the existing methods was entirely desirable and over several years an altogether different technique was devised. This formed the basis for the method now perfected at The British Hernia Centre over many tens of thousands of cases.
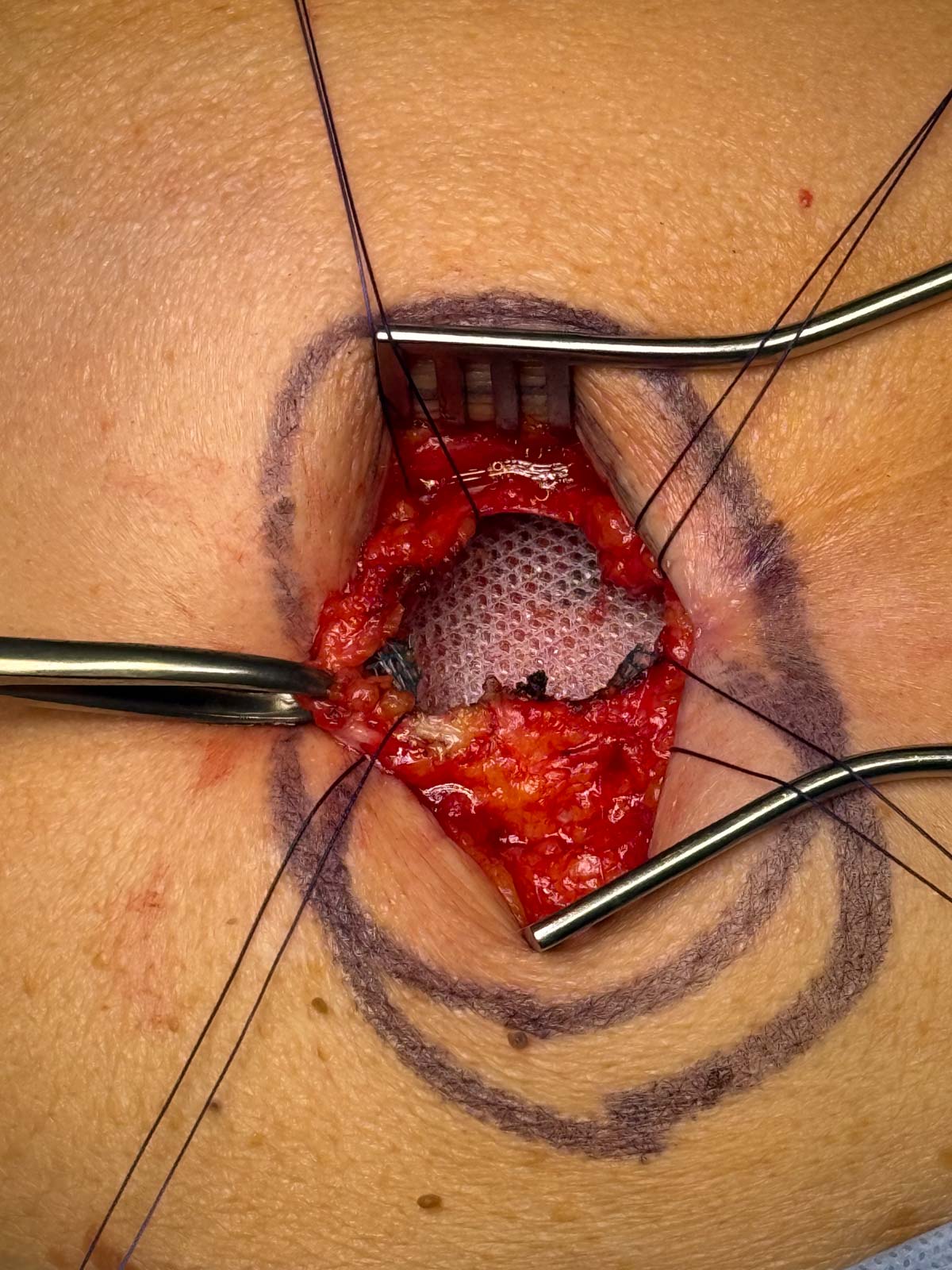
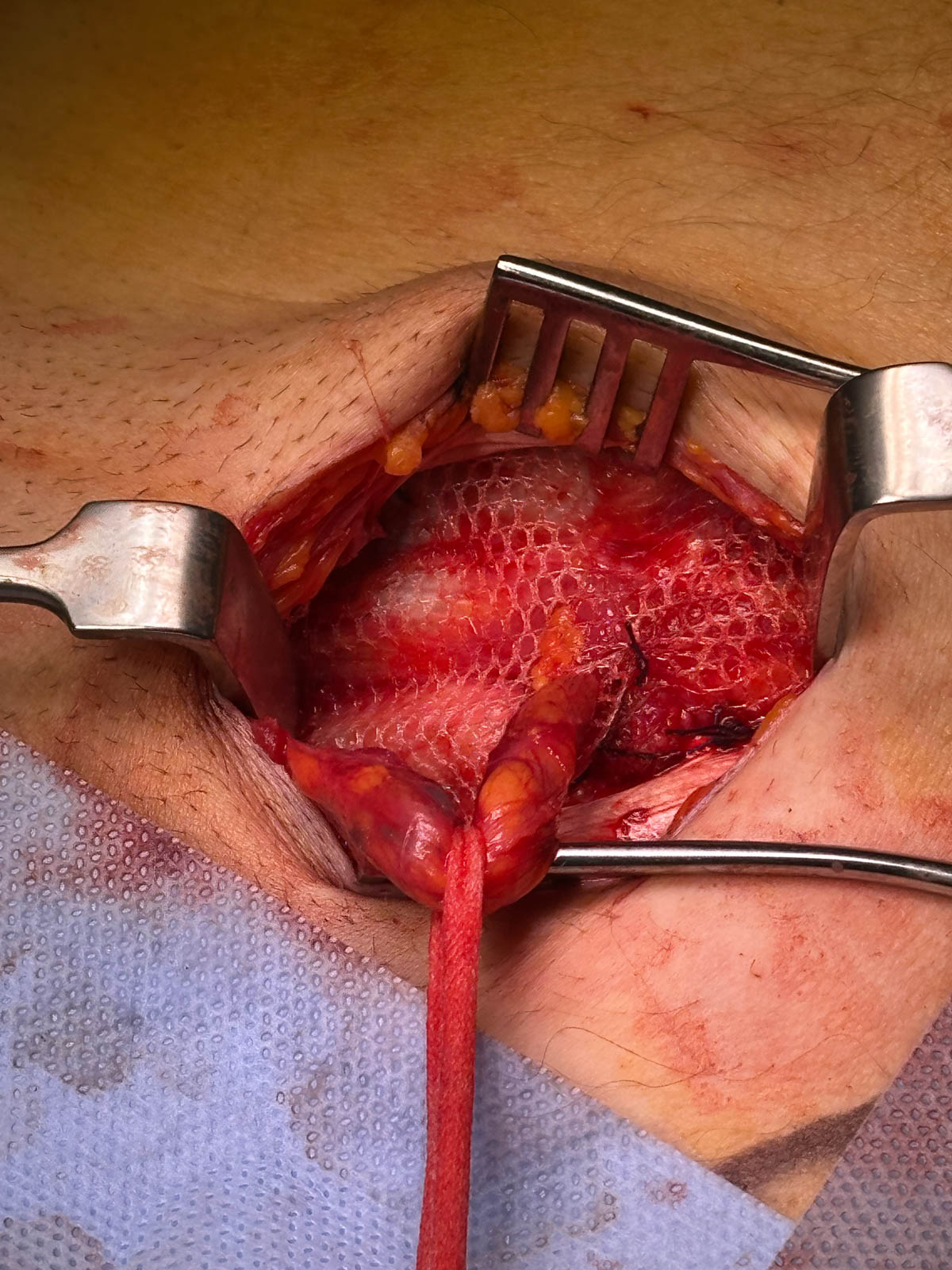
Under local anaesthesia, a small incision is made over the site of the hernia.
The peritoneal bulge is returned to where it belongs, but the repair is achieved by placing a piece of fine (inert and sterile) mesh at the opening in the tissue. This is firmly held in place and the outer incision closed. The whole operation takes minutes to perform.
Unlike other techniques, even those now using mesh, our approach does not require any stitching together of the muscle tissue at all, thus eliminating the tension induced by other methods.
The healing process starts to take place immediately whereby, (sensing the presence of the fine mesh) the muscle and tendon send out fibrous tissue which grows around and through the mesh, incorporating it in a way similar to the placing of the steelwork inside reinforced concrete. It is not a “patch” stuck on the outside, (as is relatively common with mesh repairs) but a total, tension-free reinforcement inside the abdominal wall itself. The results are also similar to the concrete analogy, in that the mechanical load is spread over the whole area, precisely at the area of weakness, rather than on high pressure points of stitching through the deep, sensitive tissue with older methods.

When performed correctly, this technique requires no bed-rest, even after the operation. The patient is able to walk away from the theatre immediately after surgery. The mesh itself is made of the same material as surgical sutures (stitches), inert and sterile and there is no negative interaction or rejection with the surrounding tissue. It is very light in weight and the patient is unaware of its presence.
The technique was originally devised as a much-needed alternative to restitching failed hernia operations (i.e. recurrences) done the old way. It was then realised that, as the technique was so very successful with recurrent hernias, it should be used for first-time repairs and thus avoid recurrences altogether. Typically, with this technique:
- A painless operation that takes minutes to perform
- No need for general anaesthesia
- No need for bed-rest, even after the operation
- Home the same day
- Back to normal extremely quickly (back at work within days)
- All kinds of sport possible afterwards
- Most reliable against recurrence for life
- Advanced age no longer a barrier
To see typical recovery experiences afterwards click here (opens in a separate window)
The papers we have had published in the academic journals, plus the press and broadcast publicity surrounding the success we achieve with our technique has encouraged many, if not most surgeons to use mesh now, rather than stitching. However, not only are there several different types of mesh in use, both in material and in construction, but there are several ways of using mesh and many levels of training and experience and the results vary enormously.
NB: The results we refer to, apply to our own techniques, performed by our own specially trained and experienced team of consultant surgeons.
Academic References:
- A unique wealth of papers by the Surgeons of The British Hernia Centre in support and evidence of the techniques developed and described have been published in the world’s leading academic journals.
- An extract appears on the menu to the left, under Academic Publications
Tension-Free Mesh – Is It Safe?
YES IT IS! This is why…
There have been reports of problems, mainly originating in the USA, with the use of mesh in certain types of surgery.
We will not comment here on those reports other than to say that they related to operations concerning female internal problems such as prolapses and matters connected with internal organs such as the bladder, vagina, urinary incontinence and so forth.
Subsequent publicity extended to the use of mesh in all other kinds of surgery, including hernia.
We need to make it perfectly clear that the mesh we use and the open techniques we employ are in no way implicated or involved in these matters.
There are several reasons for this, not least due to the anatomical differences between a hernia and, for example, a vaginal prolapse. Primarily, it needs to be understood that in hernia repair (using our technique) the mesh should not come into contact with anything significant other than the muscle and tendon tissue that has herniated within the abdominal wall structure.
The internal organs, contained within the peritoneal cavity, are not even touched in the normal course of this procedure. This applies to both genders. There is not normally any need or risk of penetrating the peritoneum (the membranous sac that contains the internal organs).
It is important to distinguish between (a) the two very different types of surgery and (b) to recognise that the claimed problems associated with the above publicity do not apply at all with the highly specialised hernia repair we perform in the country’s leading specialist hernia centre. We stress that the above only applies to our technique of repair and that not all operators employing mesh use it in the way we approve or describe.
The British Hernia Centre bases its opinion on our experience of many tens of thousands of cases over 3 decades and not a single case suffering these complications. That we, the biggest and most experienced users of surgical mesh in hernia repair have not suffered these problems suggests that what is causing the described problems is not the use of mesh itself at all.
Perhaps the way some others are using it is a factor, we can only speculate in the absence of any clinical evidence. Our unrivalled specialised experience of this hernia repair shows there is no finer, less problematic or safer way to repair abdominal wall hernias than the approaches we describe.