These hernias can all be called primary midline abdominal hernias.
Umbilical (navel) hernias occur actually in the middle of the navel. The inside of the navel sticks out. Sometimes the swelling is just above the navel so you will see a swelling just above the umbilicus. In fact you can get a hernia anywhere down the middle of your abdomen, from navel to breast bone.
When they occur a bit higher up they are called epigastric hernias. So these hernias always occur in the midline, straight down the middle, because they come out between the two rectus muscles. The lump may sometimes seem to be off to one side, but the actual defect (the hole) is always in the midline.
What would I see?
A bulge or lump beneath the skin. It can vary in size, from the size of a small grape to a large grapefruit. It depends how big the hole becomes and how much pushes out.
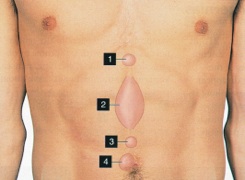 KEY
KEY1. Epigastric
2. Diastasis**
3. Supra-umbilical
4. Umbilical
** A Word About Diastasis
Diastasis is of Greek origin (διάστασις) and means ‘separation’. The Latin derived word is ‘divarication’.
In this context, it describes a situation where the two vertical muscles on the front of the abdomen separate down the middle. The thin line, or membrane between them stretches, but there is no hole. This is not a hernia.


How do I know if I have Diastasis/Divarication?
Typically everything looks normal when you are standing, maybe a bit of a bulge or prominence, but when you sit up or get up from a lying position you see a vertical ridge running from the breast bone to the navel. It can be quite prominent and sometimes very alarming, but a Diastasis or Divarication is not a hernia.
In fact attempts to correct it with surgery are usually unsuccessful.
Problem
Some call it a ‘ventral hernia’ – this worries and confuses patients and makes them think they need an operation. A prime example of the need for an expert diagnosis and sound advice.
So if it is not a hernia but a Diastasis/Divarication, our advice is to leave it alone.
When it is a hernia, what is the lump?
It is usually fat that lies beneath the muscle (part of our natural padding). Sometimes though, it may be intestine, and if that gets trapped then you have a problem. (See Strangulated Hernia)
Repair it or ‘wait and see’?
You should repair it as soon as possible.
These hernias can be relatively painless but if left alone they always enlarge. Like all hernias, if left alone they:
a) run the risk of strangulating
b) are more difficult to repair
(See also Is ‘no treatment’ an Option?)
Best repair?
Using mesh gives the best, most secure repair, but it has to be done properly.
Our experience proves that the mesh should be placed beneath the split or hole. Putting it on top, a commonly used approach, can lead to all sorts of problems such as fluid accumulation under the skin and infection.
Open or keyhole repair?
Both work well. Laparoscopic (keyhole) repair though, has two problems:
1. You are making three holes to fix one. Only worthwhile if the hernia is fairly large, because each of the holes has the potential to become a hernia.
2. The mesh is put inside the abdomen and can cause problems if the intestine sticks to it.
See also the section comparing Laparoscopic hernia repair and open mesh repair.